Surgical Robotics archives vol.2.
Imperial College has been a stronghold of European surgical robotic development from the very beginning. They started medical robotics in the mid-1980s under Prof. Brian Davies' leadership. Their first robot was the Probot, a 'prostate robot system (first tried clinically in April, 1991 and up to 1993 applied to 5 patients) which have resulted in a new Science Engineering Research Council funding initiative. "The clinical use of the automated prostate resection system in 1991(l)
was the result of four years of research and development by the Imperial
College Robotics Centre together with the Institute of Urology.
Prostatectomies involve the removal of some or all of the adenomatous
growth of the prostate gland which can cause restriction or blockage of
the urinary track. A transurethal resection of the prostate (TURP), is
carried out by the insertion of a resectoscope down the urethra, through
the penis, in order to remove a roughly conical volume of prostatic
tissue . This is a very common procedure and is considered to be a safe
operation. However, it is lengthy and requires extensive training and a
high level of skill. As carried out by diathermic cutting, using a
tungsten wire loop conducting a high frequency, high voltage electrical
current, it brings the risk of absorption of the hypo-osmolar fluid used
to irrigate the operation. This may result in an increase in morbidity."
They also ran a knee surgery project (funded by a London Hospital) "for a robotic device to machine the bones of knees for prosthetic implants; "the feasibility of using robotic systems for knee surgery. Reasons for the use of robotic systems include improved accuracy and the possibility that the operation time may be reduced. Furthermore there is the potential for a minimally invasive procedure. This will require the insertion of relatively small unicondylar prostheses placed through small incisions either side of the knee. A robotic system is necessary to achieve the complex but precise motions that are required. At Imperial College, a special purpose small reach robot system is being constructed, which can be mechanically constrained so that it can not damage either patient or medical staff".
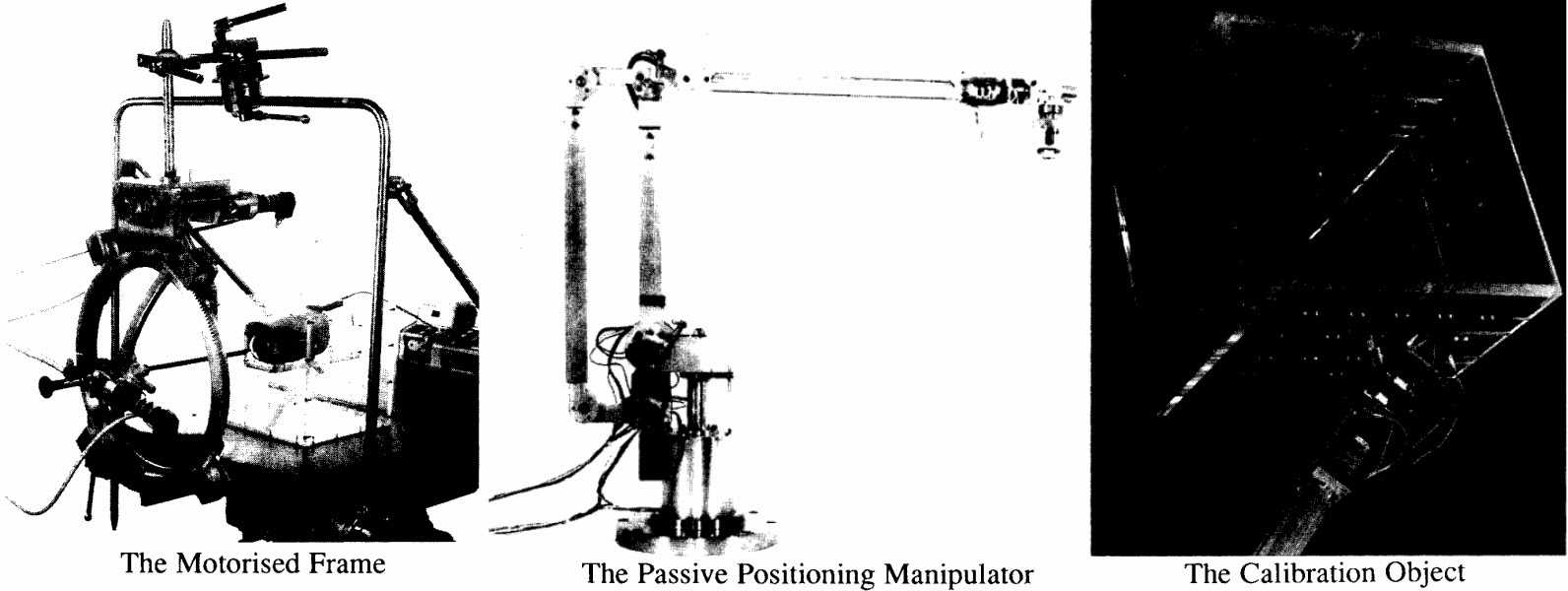
Furthermore, they experimented with a passive manipulator arm with electromagnetic brakes which is used f o r kidney biopsy in conjunction with a specially adapted C-arm X-ray machine that can give 3D quantitative measurements: "The passive manipulator under development at the Imperial College Centre for Robotics consists of a 5 DOF anthropomorphic arm designed to accommodate a variety of sterilizable endeffectors. such as biopsy needle guides and endoscope fixators. The arm is intended for direct mounting onto the operating table and is counterbalanced for nearly static behaviour. The arm's joints are equipped with potentiometers for angle measurement, interfaced to a PC via a 14-bit AjD card. The 5 DOF design facilitates the end-effector's manual placement in specified configurations. a task that can be difficult with 6 DOF manipulators. This is because the desired end-effector configuration is not always fully specified, as a number of surgical tools (needles in particular) are axisymmetric and thus indifferent to rotation about their main axis. In order for the arm to hold a tool in a fixed configuration, each joint is equipped with an electromagnetic brake. To ensure operational flexibility. brake activation is under dual control, i.e. software driven and footswitch activated. The three major axes are also equipped with mechanical locks, intended for application once the desired entry configuration has been finalized. The arm's rigidity is further enhanced by the four-bar-link configuration of the longer "reach" links."
Source: IEEE
See the previous post on Historical Surgical Robots here.
Source: IEEE
See the previous post on Historical Surgical Robots here.


Comments